Neville Martin started working at Royal Adelaide Hospital in 1958, with a background in Radio Broadcasting and trained in Television Engineering. Below is his paper presented to the 45 years of Cardiac Surgery in South Australia – “Biomedical Backup: Biomedical Engineering”.
Biomedical Backup: Biomedical Engineering
We are hearing today about the achievements surrounding the evolution and development of Cardiac Surgery in SA. This pioneering and development brought great health benefits to our community. Also, being the first to employ a significant amount of (and for the time) complex technology, it also introduced, as a fringe benefit, an activity to SA which was to develop into what we today know as biomedical Engineering. This activity subsequently developed to service a wide range of medical specialities, also adopted by other hospitals and regional services – but Royal Adelaide Hospital Cardiac pioneered it in South Australia.
Having imperfect hindsight, all that follows are recollections of early days – accuracy is not allowed in the way!
As the need for specialised equipment appeared, so did the need for some-one to change radio valves (otherwise known as vacuum tubes), solder wires together, assemble apparatus, diagnose electronic misbehaviour, as well as put in place and run electronic equipment where needed. Those who remember, will recall that electron valve equipment worked reliably on a fine day with a following breeze!
Royal Adelaide Hospital Cardiac Clinic
In September 1957, in “the Advertiser”, the Royal Adelaide Hospital advertised for a “Cardiological Technician” to “assist in the use and maintenance of electronic and other equipment in Cardiac Clinic”.
In 1958 we saw the early days of (Black and white) television broadcasting in South Australia.
In March 1958, with a background Radio Broadcasting and trained in Television Engineering, I commenced duties at RAH Cardiac Clinic under the auspices of the Honorary Cardiologists Dr Eric Gartrell and Dr John McPhie and under the good guidance and Support of Sister Kath Bonnin and her colleagues.
Cardiac Clinic was then located in the Flinders Ward building which stood adjacent to where East Wing was subsequently built.
ECG Recordings
Here I was tutored in the mysteries of ECG recording and the ECG waveforms (good & bad) and also sent to spend some time at the Royal Prince Alfred Hostile, Hallstrom Institute, in Sydney where I was to see and learn about Cardiac Investigations and Surgery.
Cardiac Clinic had recently been equipped with the Adelaide-made Both model K direct-writing ECG machines, replacing photographic recording ECGs and associated dark room processing etc. A great mentor to me at this time was the late Don Both whose premises were nearby in the now disappeared Tavistock Street.
At this time, ECG and blood-pressure monitoring and photographic recording equipment was employed for investigatory work being performed by Dr Hugh Gilmore (of the Department of Medicine) in the X-Ray Dept, and for surgery by Mr Sutherland in the original “Thoracic Theatre”.
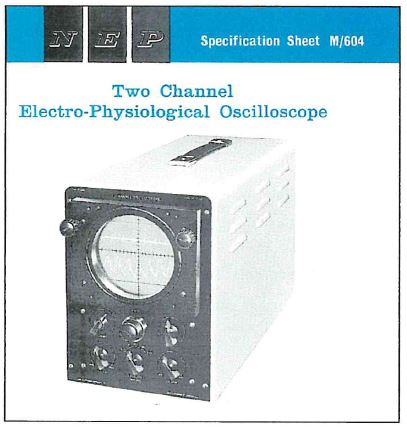
The following 5 pictures show the London-made equipment:
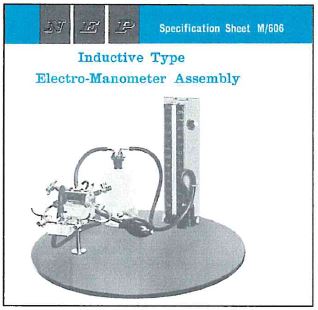

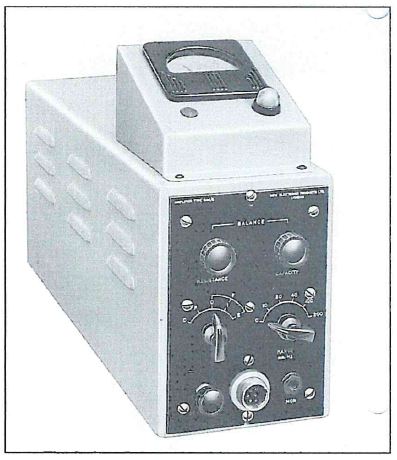
This apparatus lived in two large hand-trucks and was moved back and forth on need to either the X-Ray Dept or Thoracic Theatre and then set up.
X-Ray Department
In the X-Ray Department, this was the time of fluoroscopic imaging and before the days of image intensifiers. As one could be facing one way or another, operating equipment in this environment involved wearing for long periods, lead aprons both fore and aft and light adjusting goggles (perhaps I looked somewhat like Darth Vader – some later BME staff might agree!). All recordings made were subsequently photographically developed using the then resources of Clinical Photograph y who in turn shared facilities in the IMVS. It was here that the long time alliance with Bon Fuller, head of the existing IMVS Instrumentation (Engineering Department) can about. Also existing was the Hospital’s Surgical Instrument Technician Department, headed by Herbert Zeitz. This important and helpful group was much later to become part of the Bio-Medical Engineering Department.
1958 also saw the return of Dr Peter Hetzel from the May Clinic. Flowing from this, the scope of cardiac investigations increased and over the ensuing months, proposals by Mr Sutherland, Dr Hetzel and Dr McPhie for the development of open heart surgery rapidly brought about additional staffing together with the planning and commissioning of specialised equipment.
Heart-Lung bypass Surgery
Alterations to Thoracic Theatre were implemented to accommodate heart-lung bypass surgery. A diesel emergency power generator (the first in the hospital – much to the chagrin of ETSA) was installed as well as special wiring and intercommunication facilities.
A central electronic monitoring and recording room was created and equipped.

The remote monitoring equipment, manufactured by Sanborn (USA) was housed in a 6 foot rack-cabinet. Sanborn were later absorbed by Hewlett Packard. Multi-channel blood-pressure, multichannel ECG, ancillary channels with 4-channel display. Again, photographic recording was employed. In a concept suggested by Dr Hetzel from his Mayo Clinic experience, concealed wiring was installed form the rear of equipment through to the theatres. A dedicated, small, ECG monitor, linked into the system, was provided for the use of Dr John Stace and Dr Pauline Daniels the anaesthetists.
As mentioned, multiple cables were needed from the central monitoring equipment (recording room) to the several operational sites in the building. An innovation here was the installation of overhead connection boxes at these sites thus minimizing floor clutter. A great help in this was Mr Cas Herbst, then electrical engineer with the Public Building Department.
However, the specialised instrumentation cables had to be run through the roof-space! By this time, Neil Pressley, who was to become the long-term and dedicated heart-lung machine technician and carer, had joined the team. He and I clambered and crawled through the roof-space and installed the specialised cables ourselves. I remain most grateful for his help.
Successful equipment tests and trail runs followed and the rest is history.
Cardiovascular Investigational Unit
In 1960, the Cardiovascular Investigational Unit was formed, headed up by Dr Peter Hetzel. As well as medical specialties, the Unit included services such as electronics technology and physiological technicians and the like. The mergence of the Medical Electronics identity gradually followed.
I followed the construction of East Wing with interest, the site being close to the Botanic Gardens and the lakes fed by First Creek. Surprise! The excavated site promptly filled with water! Some time later, after the completion of East Wing, there followed the RAH rebuilding programme involving the new theatre, Administration and Outpatients Block.
In MES, we had been joined by Bert Stacey and later by Robert Wiseman.
East Wing
The rebuilding program brought about the relocation of Cardiothoracic Surgical Unit to the East Wing.
The relocation of theatre again involved specialised wiring and the reinstallation of the original ‘Sanborn” monitoring and recording system to its new recording room in the East Wing.
And this is how it looked:
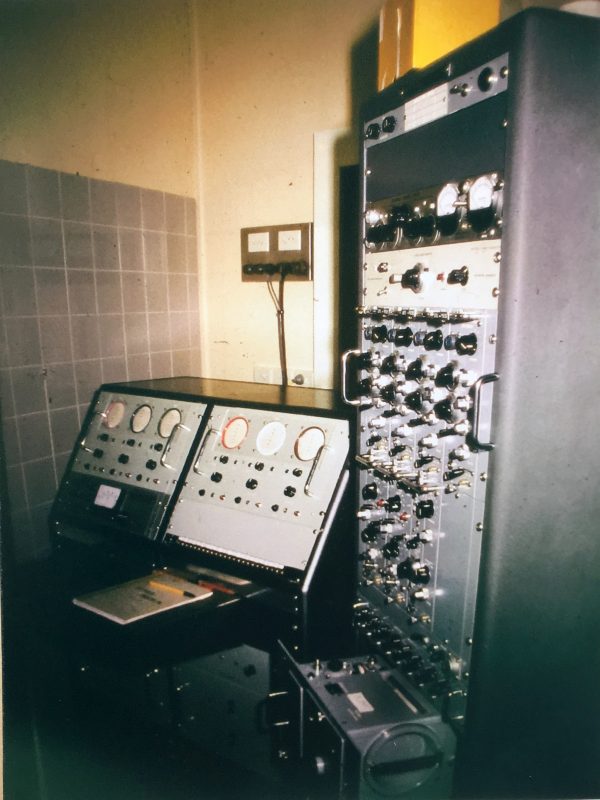
The original small four-channel monitoring oscilloscope had become unreliable and was replaced. Its replacement, a six-channel oscilloscope was constructed in-house at modest cost. The resulting avialble cabinet space was occupied by oimeter equipment. Multi-channel blood presure, ECG, oximeter channels were still recorded by photographic recorder.
Also, a Recovery ward had been established and this had its own monitoring equipment which Medical Electronics also looked after.
In the Cardiac Investigation area, radiological equipment had been upgraded and now included image intensification. An adjacent recording room was created where rack-cabinets of monitoring equipment had been assembled by Medical Electronics giving:

- several channels of blood pressure,
- Dye densitometer – cardiac output,
- ECG,
- ‘Honeywell’ direct-writing recorder employing ultra-violet light and photographic paper. Note the NEP 2-channel oscilloscope still in service and the TV screen to display image intensifier images.

‘Statham’ resistance blood pressure tansducers were now used in both Cardiothoracic Surgery and Cardiac Investigation and had been for some time, indeed, since the introduction of the’Sandborn’ equipmetn in Thoracic Theatre.

In the CVIU radiological room – Sanborn/Hewlett Packard multi-channel, large-screen physiological oscilloscope and image intensifier TV screen.
Then came North Wing planning of the Coronary Care and Intensive Care Units. Planning of this area involved Dr Hetzel, Dr Morris Sandow (Director of Anaesthesia) Mr Bob Blewitt (PBD) and myself. With the completion of North Wing, which had a planned, dedicated Coronary Care area, as well as an Intensive Care area), the need for more equipment arose. Because of tendering formalities, new equipment was somewhat delayed and temporary ECT monitors on trolleys employed.

Q4 Coronary Care – temporary central station – note the old NEP oscilloscope pressed into service again – patient call system – direct-writing ECT recorder with patient selector switch/heart rate meter.
Then the new equipment arrived.
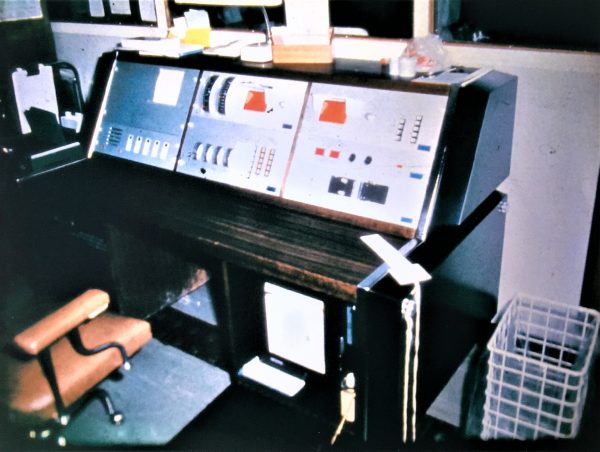
The first, formalised, Q4 Coronary Care monitoring system central station (Telectonics, Australai). A typical built-in modular bedside unit.

Theatre Block
On the completion of the Theatre Block, Cardiovascular Investigation moved into its newly equipped home there. Under the directorship and continuing support of Dr Hetzel, Medical Electronics was also housed in the same area. In the procedures area, the latest radiological equipment with image intensification was installed. Again, monitoring equipment was commissioned in a central recording room.
With the evolution of technology we saw the arrival of implanted cardiac pacemakers. Dr Waddy frequently performed implantations, whilst Bert Stacey of Medical Electronics assisted by way of measuring the recording pacemaker performance data which he subsequently then followed up, recorded, and reported on thought out the pacemaker life.
I have touched only on a very small part of 45 years. The early ones certainly being exciting and adventurous. For the electronic backroom boys & girls, eventually, growth and continuing support from Dr Hetzel, brough about devolution into a new department, in its own right – biomedical Engineering – but one which continued its important Cardiac Association.
Thank you for the honour of being invited to speak today.